It is not unusual to have some unexpected (unscheduled) bleeding in the first 3 to 6 months after starting or changing HRT, even if the last natural period was many years ago. Every woman should be reviewed after their first 3 months on HRT and if the bleeding shows no signs of improving, the HRT can be adjusted to try to settle it.
Any bleeding that persists after 6 months on HRT, or starts once the patient has been on HRT for 6 months, does need to be investigated. Very heavy or painful bleeding, post-coital bleeding (after sex) or bleeding associated with other worrying symptoms would need to be investigated sooner.
The first port of call would be the GP who can take a detailed history to check:
- are they taking the HRT correctly e.g. do the patches stick on properly or is the patient taking the right amount of progesterone to protect the lining of the womb?
- how long have they been on HRT and have there been any changes in treatment?
- are they using unregulated bioidentical HRT eg transdermal progestogen cream?
- when was their last smear?
- do they need a vulval, vaginal and cervical examination with swabs?
- any risk factors for endometrial cancer (see below)?
- do they need a gynaecological referral for further assessment?
We now have a joint national guideline on how to manage unscheduled bleeding on HRT (published April 2024) although it may take a while for the recommendations to be adopted locally. https://thebms.org.uk/2024/04/joint-bms-bsge-bgcs-fsrh-girft-and-rcog-guideline-on-management-of-unscheduled-bleeding-on-hrt/
Most unscheduled bleeding on HRT is due to the HRT but it is very important to exclude vulval, vaginal or cervical pathology, endometrial polyps, endometrial hyperplasia, endometrial cancer, fibroids and ovarian cancer.
Risk factors for endometrial cancer include the use of unopposed estrogen in women with a uterus, obesity, Type 2 diabetes, not having children, a late menopause, polycystic ovary syndrome, previous hyperplasia and tamoxifen use. This is the 4th most common cancer in women in the UK. Women on continuous combined HRT have a lower risk of endometrial cancer than women not on HRT.
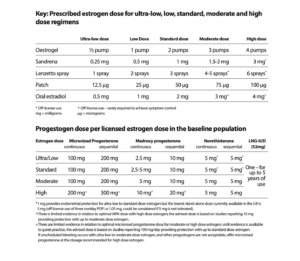
It is very important that women take the progestogen part of HRT (for endometrial protection if they still have a uterus) as prescribed for as long as they are taking estrogen. Some women are reducing or stopping this part of their HRT, putting themselves at risk of endometrial cancer. The management of unscheduled bleeding on HRT guideline (link above) also includes advice on the dose of micronised progesterone needed depending on the dose of estrogen prescribed and any risk factors for endometrial cancer.